In colloquial terms, a broken heart does exist, but in the cardiological sense, in terms of pathophysiology, the broken heart syndrome refers to a complex clinical entity. It got its name from an octopus trap – and that’s not all that is unusual about this reversible heart condition.
It almost exclusively occurs in women. It most commonly occurs as a result of suddenly intense emotional reactions, which is why it is also called stress cardiomyopathy, stress-induced cardiomyopathy, Takotsubo cardiomyopathy, or broken heart syndrome.
Takotsubo cardiomyopathy was named in Japan after the traditional Japanese octopus trap, known as takotsubo vessel, which is lowered into the sea. As the heart has the same shape as this fishing trap on ultrasound, Japanese doctors named the stress-induced cardiomyopathy after it.
So, a broken heart is actually the syndrome known as stress cardiomyopathy.
When was broken heart syndrome recognized in medicine?
Takotsubo cardiomyopathy (broken heart syndrome) was first described in 1991 after an earthquake in Japan. Scientists, while studying how such natural disasters affect people, discovered that after earthquakes, there are often more deaths that appear to be heart attacks but are not actually so. Stress cardiomyopathy is characterized by transient ballooning of the apex of the left ventricle, giving it the appearance of an ampulla or the aforementioned octopus trap.
It is a relatively new syndrome that has entered widespread clinical practice in the last, I can freely say, more than 20 years. Changes in the heart muscle located in the apex of the left ventricle have been described. Pathophysiologically and histologically, stress cardiomyopathy can occur in various situations of increased stress. Whether it is infections, autoimmune diseases, intense physical exertion, extreme situations, in any case, any form of significant stress in a female individual susceptible to these factors can hypothetically lead to the syndrome – stress cardiomyopathy, emphasizes Dr. Svetislav Mališić – cardiologist.
Rees WD et al. first reported in 1967 that death and the loss of a close relative increase the risk of death from this syndrome by seven times within one year of the occurrence of this stressful event.
Engel George, in 1971, described sudden and rapid cardiac death following emotional stress and identified 8 groups of precipitating factors as possible risk factors:
- Stress caused by loss or death of a close person.
- Acute grief.
- Threat of losing a close person.
- Mourning or marking the anniversary of the loss of a loved one.
- Loss of status or self-esteem in society.
- Life endangerment or threat of injury.
- Period after the cessation of danger.
- Reunion, triumph, or happy ending.
According to Engel, these events induce neurovegetative reactions, which are particularly pronounced in individuals with pre-existing cardiovascular diseases.
What is stress cardiomyopathy?
Symptoms occur, classic symptoms like those of heart failure – acute cardiac decompensation. It’s as if the patient is in a life-threatening situation during these episodes. This condition can also lead to cardiac rhythm disturbances and can even be a life-threatening condition if not recognized in time.
Is the name stress cardiomyopathy due to stress?
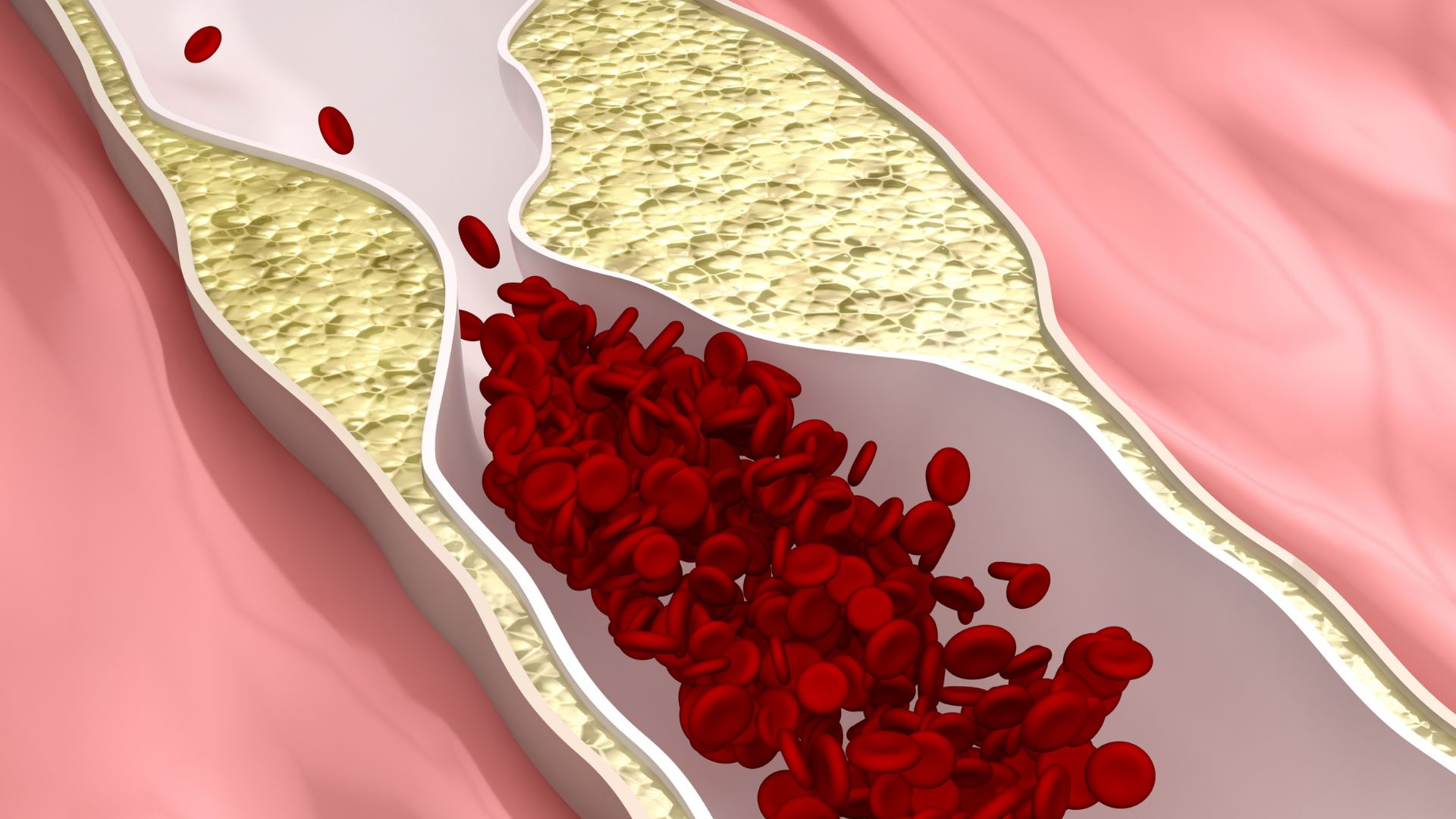
Exactly, when the body is under stress, various hormones are released that affect all organs, not just the heart, and they can lead to changes in the muscle of the left ventricle (if the person is susceptible to it). It is known that stress leads to the activation of the hypothalamic-pituitary-adrenal and sympathoadrenal systems. However, the impact of stress on the cardiovascular system is not yet fully understood. Major psychosocial factors such as depression, anxiety, social isolation, and other stressors can lead to myocardial ischemia, disturbances in heart rate, platelet activation, dysfunction of coronary artery endothelium, and even cardiomyopathy.

Is Broken Heart Syndrome the same as a heart attack (myocardial infarction)?
Patients often exhibit a similar clinical presentation and symptoms to those with acute myocardial infarction (AMI): chest pain, shortness of breath, abnormal ECG findings, reduced ejection fraction, elevated troponin (TnT, TnI) and creatine kinase levels, but without occlusion, stenosis, or spasm of the major coronary arteries. However, unlike a heart attack, Takotsubo is a reversible syndrome, as most parameters and symptoms normalize in 95% of patients within 1-6 weeks.
The etiology of this disease is still unknown and clearly multifactorial. It is evident that individual differences exist, and not everyone is equally susceptible to developing this cardiomyopathy. It is hypothesized that genetic risk factors in combination with other factors may contribute to the onset of the disease. In 20-60% of Takotsubo patients, some form of psychological disorder, such as depression and anxiety, has been previously diagnosed. It is known that these disorders affect catecholamine metabolism, particularly their uptake, and that depressive and anxious patients have increased activity of the endocrine system, making them more susceptible to stress.
Diagnosis and Symptoms of stress cardiomyopathy
Diagnosis is established through a conventional cardiological examination, ECG, and especially an echocardiogram where specific morphological changes in the apex of the left ventricle, resulting in the “broken heart” syndrome, can be observed. Fortunately, stress cardiomyopathy is treated and managed with modern therapy, and in most cases, it resolves quickly.
Characteristics of Takotsubo cardiomyopathy:
- Chest pain and shortness of breath following intense stress (emotional or physical)
- Abnormal electrocardiogram (ECG) and changes mimicking a heart attack
- No apparent obstruction of the coronary arteries
- Impaired left ventricular movement
- Ballooning of the left ventricle
- Recovery within one month
Is death possible from a broken heart?
Most abnormalities in systolic function and wall motion resolve within one to four weeks, and the majority of patients fully recover within two months. Death is rare, but cardiac arrest occurs in about 20% of patients. Treatment involves the use of diuretics, medications that improve cardiac muscle contraction, and other drugs. Less common complications include arrhythmias (abnormal heart rhythm), obstruction of blood flow from the left ventricle, and rupture of the ventricular wall.
If you experience any symptoms such as rapid fatigue, shortness of breath, heart palpitations, ringing in the ears, choking sensations, or leg swelling, it is time to visit a cardiologist and undergo a comprehensive heart examination. At Pulse Cardiology Center, we offer complete cardiological care according to international standards.